When a Simple Fall Isn’t So Simple
What Did we See?
A 78-year-old woman arrived at our emergency department after what sounded like a trivial fall
— she was simply trying to sit and missed the chair. But what followed was far from trivial. She
had pain and swelling in the right shoulder and hip, complete motor and sensory loss in the right
upper limb, and absent brachial and radial pulses. On initial evaluation, she also couldn’t bear
weight on her right lower limb. She was rushed to a level 1 trauma center in Kathmandu Valley.
Radiographs showed a displaced proximal humerus fracture and an unstable intertrochanteric
fracture. But it was the CT angiogram that revealed the real danger — a complete disruption of
the axillary artery, with no distal flow. The upper limb was ischemic, neurologically silent, and
at real risk.
We made a diagnosis of closed displaced 2 part Proximal Humerus fracture right side (Neer 2
part) with axillary artery injury and Global Brachial plexus injury with ipsilateral intert-
trochanteric femur fracture right side (Boyd and Griffin type 3).
What Did we Do?
We moved fast. A multidisciplinary team — orthopedic, vascular, and anesthesiology — was
mobilized. Through a deltopectoral approach, we found a 3 cm laceration in the axillary artery,
entrapped along with the brachial plexus cords between the humeral head and shaft. Using a
reversed saphenous vein graft, the CTVS team repaired the artery. Smooth K-wires were used to
stabilize the humeral fracture quickly and minimize soft tissue trauma.
The intertrochanteric fracture was fixed with a dynamic hip screw in a staged procedure. Early
neurological recovery followed: finger flickers on day two, improving to partial wrist and elbow
movement within a week.
What Did we Learn?
This case was a powerful reminder that mechanism does not always predict magnitude. low-energy fall in an elderly patient can still lead to devastating injuries, especially in the
presence of osteoporosis.
I learned:
• Always assess neurovascular status thoroughly in proximal humerus injuries.
• Loss of distal pulses is a surgical emergency — time matters.
• Simple imaging is not enough — CTA should be done when vascular injury is
suspected.
• Biological reconstruction and minimally invasive fixation can offer stabilisation of
fracture and buys time for repair of vascular injury and minimizes anesthesia time in
elderly, high-risk patients.
And most importantly — don’t let the simplicity of the story fool you. A fall from standing
height can still be a high-stakes surgical challenge.
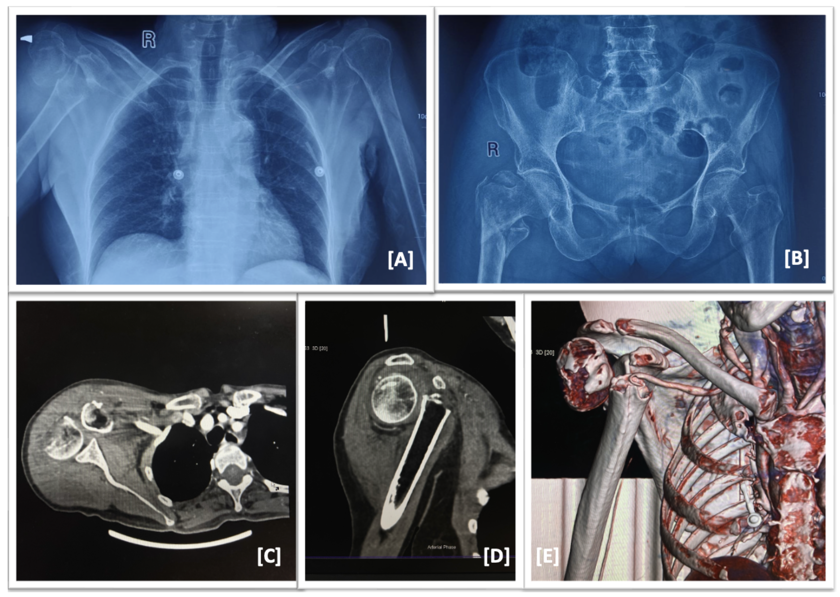
Figure 1: A,B: Plain radiographs of chest and pelvis showing right sided proximal humerus 2
part fracture and proximal femoral fracture (IT fracture, Boyd and Griffin type 3); C,D,E:
Computed tomography with angiogram showing filling defect in 3rd part of subclavian artery.
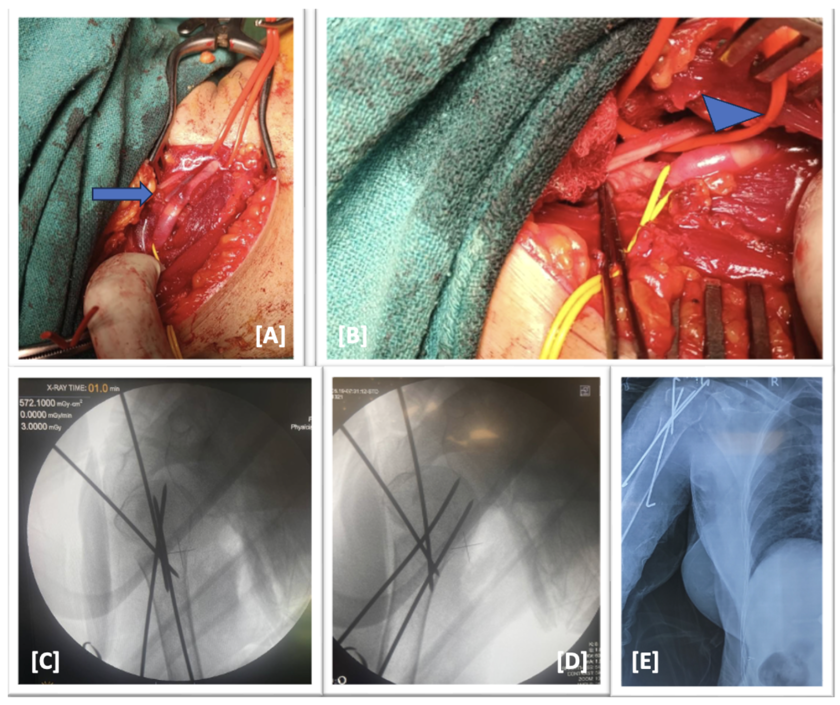
Figure 2: A: Intraoperative image showing laceration(arrow) of distal part of subclavian artery
and proximal part of axillary artery (3rd part of subclavian artery and 1st and 2nd part of axillary
artery); B: Laceration was repaired with reverse saphenous graft and floow was restored as seen
by the dilation of the grafted part(arrowhead); C,D,E: Intraoperative and postoperative images
showing fixation of proximal humerus with provisional k wires in both antegrade and retrograde
fashion as well as avoiding injury to the repaired part while achieving good anatomical
reduction.
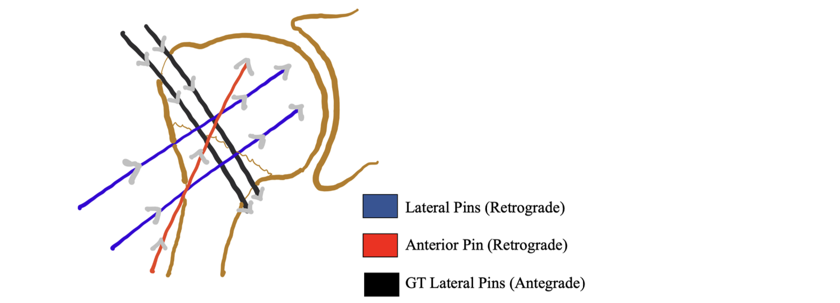
Pearls: Surgical Technique for 2-part proximal humerus fracture fixation with
provisional K-wires.
• Use 2.5 mm terminally threaded K-wires after achieving an adequate fracture reduction.
• Typically, insert three K-wires: one anterior-to-posterior and two lateral-to-medial, placed in
two planes with different angulations.
• Anterior pins add torsional stability but must be placed carefully to avoid the biceps tendon or
cephalic vein.
• Based on biomechanical data, placing two K-wires from the tuberosities into the medial
proximal humeral cortex increases construct rigidity compared to lateral pins alone.
• Lateral pins should enter at a safe point to avoid the axillary nerve, ideally at twice the head
height distance from the superior margin of the humeral head.
• Insert pins through a sleeve at 30° retroversion to minimize soft tissue damage.
• Pins should diverge at the fracture site and within the humeral head for optimal stability.
• Advance K-wires to the subchondral bone without penetrating the articular surface.
• Use fluoroscopy in AP and axillary views, including 60° external rotation, to confirm accurate
and safe pin placement
Recent Related Blogs
- No related blogs found.